Tuberculosis (TB) remains a serious problem for thousands of residents in South Africa, as the disease is often discovered too late, not because treatment is unavailable.
Application of the AI tool
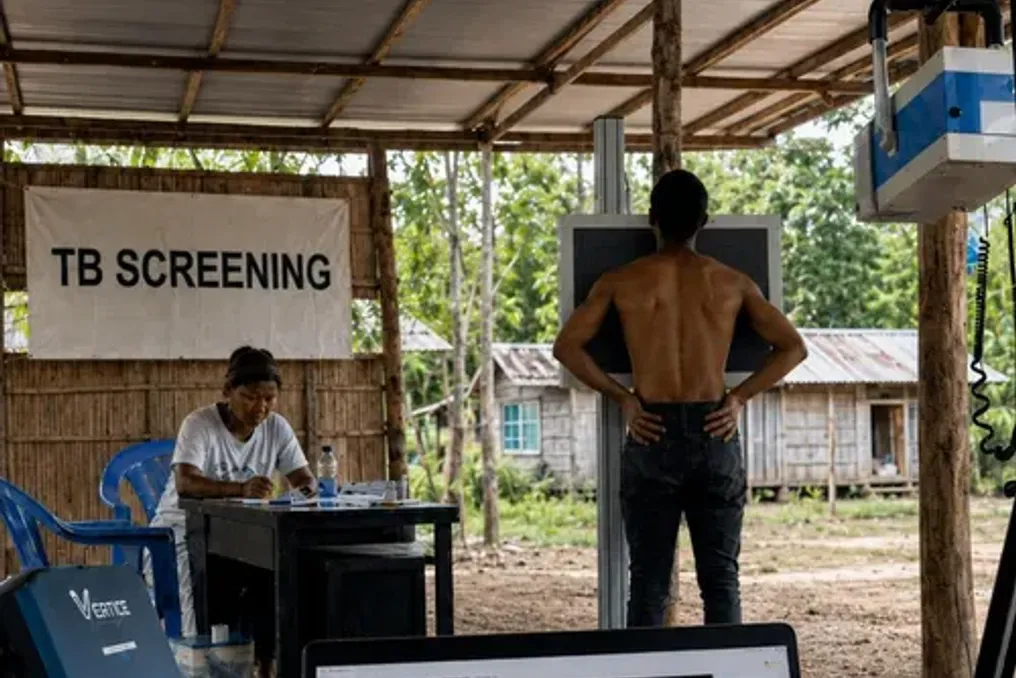
The Nexus AI artificial intelligence tool, developed in Pretoria, now helps healthcare workers identify individuals who do not exhibit obvious symptoms. This gives patients in rural areas and other underserved zones a greater chance of receiving treatment before the disease becomes life-threatening.
This tool, which is based on analyzing chest X-rays using AI, is already being used in community-level screening programs in the Northern Cape, Eastern Cape, and Durban. It allows frontline healthcare workers to identify people who might otherwise be sent home without further examination.
Motivation for developing the technology
Andries Forster, co-founder of the Pretoria-based technology company behind this development, stated that the idea arose after years of observing how people missed timely diagnosis due to a lack of specialists to interpret X-rays. Forster noted that the issue was not an isolated case but a recurring trend they observed while supporting radiology services in rural communities, mobile clinics, and under-resourced healthcare facilities across Africa.
He emphasized that simply having an X-ray machine is not enough; the ability to interpret the image must accompany the equipment and be available directly at the point of care. The need for early detection became even more apparent after a national TB prevalence survey in South Africa showed that nearly 58% of people with bacteriologically confirmed TB had abnormal chest X-rays despite lacking traditional symptoms.
How the system works and its advantages
Forster explained that many TB patients did not present as expected by healthcare workers. He stated that one cannot wait until people are visibly ill to detect lung diseases, and they needed a tool that could help frontline workers find subtle deviations earlier, regardless of the patient's location.
The technology acts not as a replacement for doctors, but as an early screening and triage tool. In about 45 seconds, it can indicate whether an X-ray is normal, contains an anomaly requiring further study, or shows signs indicative of TB. Patients who receive a positive result still undergo clinical assessment and confirmatory testing.
For people living far from medical facilities, these seconds can make a huge difference. As Forster said, for such a person, the real difference is not just that 45 seconds replaces several weeks, but that it can be the difference between one coordinated medical visit and complete dropout from the healthcare system. Without immediate analysis, a rural patient might get an X-ray and go home while the film is sent elsewhere for reporting, forcing them to travel repeatedly, spend money on transport, lose income, and wait weeks for a response.
Current use of the technology
It has been found that this technology currently supports TB and lung health screening programs conducted by the National Department of Health, the Aurum-PRO program in the Eastern Cape, the SIOC-CDT community screening initiatives in the Northern Cape and Limpopo, as well as outreach programs for homeless communities in Durban.
Forster cited an example from a screening program in the Northern Cape: a person who felt well and reported no classic TB symptoms underwent a routine check-up. Based only on symptoms, this person likely would not have been referred for TB testing. However, the X-ray revealed an anomaly suggesting the disease, prompting healthcare workers to conduct further molecular testing and link the patient to treatment before the disease progressed.
Similar experiences were recorded within mobile screening programs in the Eastern Cape and among homeless communities in Durban, where immediate screening allows healthcare workers to organize testing and counseling while patients are on site, reducing the risk of loss to follow-up.
One clinician participating in the screening programs noted the obvious impact: 'What is striking is how many patients we are now detecting who might have been missed. Without the AI alerting us to subtle findings, they would not have been referred for further testing.'


