Researchers from six different countries have published a report on the positive results of the third phase of clinical trials for the melanocortin receptor agonist—setmelanotide. This drug has shown the ability to effectively reduce body mass index and decrease hunger in subjects.
Mechanism and Causes of Obesity
Hypothalamic obesity arises from disruptions in the hunger and satiety centers located in the hypothalamus. The causes can be diverse: ranging from genetic defects in the melanocortin system (such as POMC, PCSK1, or LEPR deficiency) to the effects of pharmacotherapy (antipsychotics) or acquired damage to the hypothalamus, such as tumors, traumatic brain injuries, or inflammatory processes.
The disease itself is characterized by a number of symptoms: increased fatigue, sleep problems, thermoregulation disorders, uncontrolled overeating, slowed metabolism, and rapid weight gain. Setmelanotide, being a peptide analogue of natural α-melanotropin, became the first drug in the class of melanocortin MC4 receptor agonists. It has been used since 2020 for congenital hypothalamic obesity and has successfully passed initial trial stages for the acquired form.
TRANSCEND Phase Three Study
The double-blind randomized controlled trials of the third phase, TRANSCEND, were conducted by Christian Roth and his colleagues from the UK, Germany, Canada, the Netherlands, the USA, and Japan. The studies took place in 29 clinical centers across six countries and involved 120 people aged four to 66 years (mean age—19.9 years; 60% of participants were women).
Participants had hypothalamic obesity caused by acquired hypothalamic damage, most often craniopharyngioma. Their body mass index exceeded the 95th percentile for their sex and age (the average z-score for younger participants was 3.61 ± 1.66) or was 30 kg/m² or higher (for individuals over 18 years old, the average figure was 41.2 ± 9.7 kg/m²).
Results and Safety of Therapy
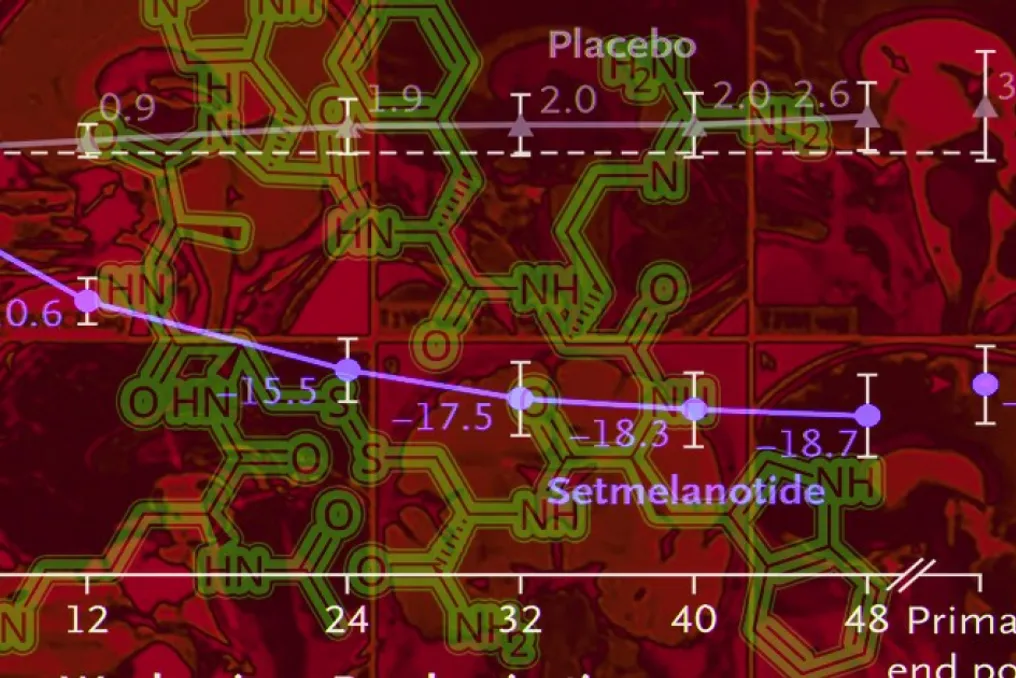
Participants were randomly assigned in a 2:1 ratio and were administered subcutaneous setmelanotide once daily in increasing doses from 1.5 to 3.0 mg (depending on body weight) or placebo. Treatment lasted 52 weeks after reaching the target dose.
Over the 52-week period, the average reduction in body mass index was -16.5% when using the active drug compared to 3.3% with placebo (p < 0.001). Furthermore, 83% of participants (compared to 21% in the placebo group) achieved a reduction in z-score of at least 0.2 (for those under 18 years old) or a five percent reduction in body mass index (for those over 18 years old) (p < 0.001).
The average change in the maximum daily hunger score on a scale from 0 to 10 was -2.73 with setmelanotide and -1.45 with placebo (p = 0.009). Among adverse events, cases were observed in 100% of the main group and 90% in the control group, including 28% and 8% serious reactions. The most frequently noted side effects were headache, nausea, vomiting, and skin hyperpigmentation.
Study Conclusions
The study confirmed that therapy with the melanocortin agonist setmelanotide can effectively reduce body mass in acquired hypothalamic obesity compared to placebo. This strengthens the hypothesis that the disruption of α-melanotropic receptor signals in the MC4 pathway plays a key role in the development of this disease.
Additionally, German scientists previously described an atypical case of severe early hypothalamic obesity in a girl associated with the overexpression of the ASIP gene due to the duplication of chromosome 20 segment, which leads to the suppression of the MC4 receptor signaling pathway. Theoretically, setmelanotide could also help in such forms of obesity.